
Silent Reflux Relief: Safe Ways to Angle Your Newborn’s Sleep Surface
The Silent Struggle: Understanding Your Baby’s Discomfort
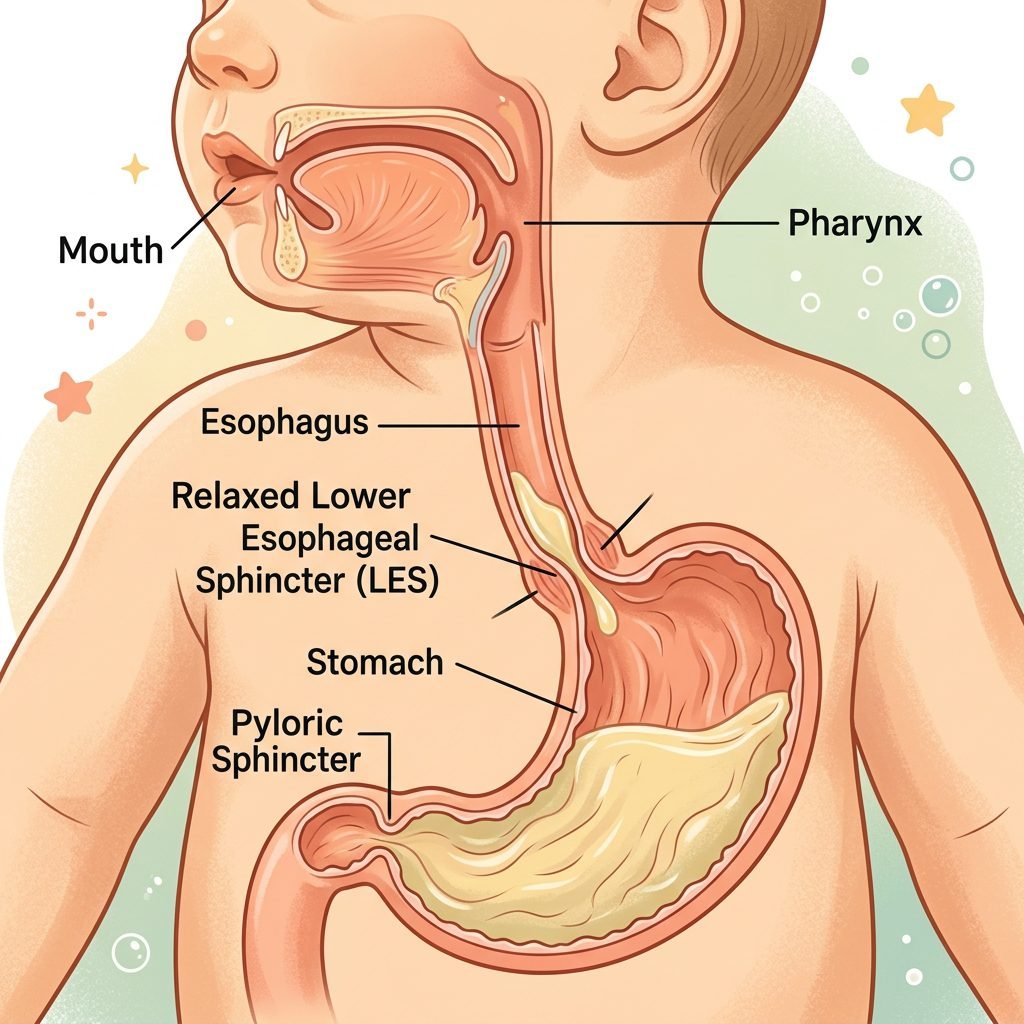
Oh, mama, I see you. I see the tired eyes, the late-night Google searches, and the heartache that comes when your sweet little one is clearly in pain, but there is no ‘spit-up’ to show for it. Silent reflux, or Laryngopharyngeal Reflux (LPR), is a challenging journey. Unlike traditional reflux where the milk makes a grand exit, silent reflux happens when the stomach contents travel back up the esophagus but are swallowed back down, causing a double-burn that can lead to arching, coughing, and inconsolable crying.
As a doula, I’ve sat with many mothers in the dark of night, wondering if they should prop up the crib mattress or buy that expensive wedge they saw online. The instinct to ‘angle’ the baby to let gravity do the work is natural, but we must balance that comfort with the gold standard of safe sleep. In this guide, we are going to walk through the ‘why’ behind the reflux, the physical techniques to ease the burn, and exactly how to manage sleep surfaces so your baby stays safe while finding much-needed relief.
Remember, sweet mama: You are doing an incredible job. This phase is temporary, and your intuition combined with safe practices is your baby’s best defense.
Recognizing the Signs: Is it Silent Reflux or Just ‘Gassy’?
The Telltale Signs of the ‘Silent’ Burn
Before we dive into positioning, we need to be sure what we are dealing with. Silent reflux often mimics other newborn behaviors, but certain patterns stand out. If your baby is struggling with silent reflux, you might notice sour-smelling breath even hours after a feed, or a wet-sounding cough that happens when they are lying flat.
- The ‘Arch and Cry’: Baby pulls their back into a ‘C’ shape during or immediately after feeding.
- Frequent Hiccups: While common in all babies, frequent, painful-looking hiccups can indicate reflux.
- Congestion: A ‘stuffy’ nose that doesn’t seem to be a cold, caused by milk irritating the nasal passages.
- Difficulty Swallowing: You might hear a ‘clicking’ sound or see baby gulping even when they aren’t feeding.
Reflux vs. Normal Newborn Digestion
Every baby has an immature lower esophageal sphincter (LES)—the muscle that acts as a lid to the stomach. In most infants, this just means ‘happy spitting.’ In reflux babies, the stomach acid is more irritating. It is vital to track these symptoms to share with your pediatrician.
| Symptom | Normal Gas/Spit-up | Silent Reflux Warning |
|---|---|---|
| Feeding Behavior | Generally calm, may pull off once | Arching, screaming, or ‘feeding-strikes’ |
| Sleep Quality | Wakes for hunger | Wakes screaming shortly after being laid flat |
| Weight Gain | Steady and on track | Can be poor if feeding is too painful |
| Breath Scent | Milky/Sweet | Sour or acidic scent |
The Safe Sleep Angle: Navigating the 10-Degree Rule

Why We Don’t ‘Prop’ the Mattress Anymore
I know the old-school advice: ‘Put a phone book under the mattress’ or ‘Use a sleep wedge.’ However, as your doula, I have to be firm: The American Academy of Pediatrics (AAP) updated their guidelines to state that sleep surfaces should not be inclined more than 10 degrees.
When a baby is placed on a significant incline (like a car seat or a wedge) while sleeping, their heavy head can fall forward, causing positional asphyxiation by kinking the airway. Furthermore, babies with reflux who are angled can slide down the mattress, potentially ending up in a position where their face is pressed against the side of the crib or their chin is tucked to their chest.
Creating a Safe ‘Micro-Angle’
If your pediatrician specifically recommends a slight incline, it must be done with extreme caution. Here is the safe way to approach it:
- Never use loose pillows or wedges on top of the sheet. Anything added to the sleep surface increases the risk of SIDS.
- Check for ‘The Slide’: If you do slightly elevate the head of the crib (under the mattress only), ensure it is less than 10 degrees. If the baby is sliding down at all, it is too steep.
- The ‘Flat is Best’ Reality: For most babies, the safest place is a firm, flat surface. We achieve ‘relief’ through pre-sleep positioning rather than the sleep surface itself.
Pre-Sleep Rituals: The ’30-Minute Upright’ Rule

Gravity is Your Best Friend
Since we want the sleep surface to stay flat and safe, the ‘work’ of reflux management happens in the 30 minutes before the baby’s head hits the mattress. This is the most critical window for silent reflux relief.
- The Vertical Cuddle: After every feed (including those 3 AM sessions), hold your baby vertically against your chest. Their chin should be over your shoulder. Avoid ‘scrunching’ their stomach; keep their torso elongated.
- The ‘Tiger in the Tree’ Hold: Lay baby face down along your forearm, with their head in your hand and legs straddling your elbow. This puts gentle pressure on the tummy while keeping the head elevated above the stomach.
- Avoid the Diaper Change Crunch: Try to change the diaper before a feed. Lifting a baby’s legs high to wipe their bottom right after a feed ‘squeezes’ the stomach like a tube of toothpaste, forcing acid up.
“Hold them close, mama. Those 30 minutes of upright time are not just for their digestion; they are for your bonding. Use this time to hum, whisper, or just breathe together.”
Feeding Strategies to Minimize the Burn

Paced Feeding and Air Management
How the milk goes in determines how much comes back up. Whether you are breastfeeding or bottle-feeding, the goal is to reduce the amount of air the baby swallows, as air bubbles trap acid underneath them.
For Breastfeeding Mamas:
- The ‘Laid-Back’ Position: Lean back so the baby is on top of you. This slows the flow of milk if you have a heavy let-down, preventing the baby from gulping air.
- Frequent Burping: Don’t wait for the end of the feed. Burp the baby every time they pull off or when you switch sides.
For Bottle-Feeding Mamas:
- Paced Bottle Feeding: Keep the bottle horizontal so the baby has to actively suck. This prevents ‘flooding’ the esophagus.
- Anti-Colic Valves: Use bottles designed with vents to ensure the baby isn’t sucking in air.
| Technique | Benefit | Best For |
|---|---|---|
| Paced Feeding | Prevents overfilling the stomach | Bottle-fed infants |
| Upright Nursing | Uses gravity during the meal | Breastfed infants |
| Small, Frequent Meals | Reduces stomach pressure | All reflux babies |
The Doula’s Toolkit: Manual Relief Techniques

Bicycle Legs and Tummy Massage
While silent reflux is an upper-GI issue, it is often exacerbated by lower-GI gas. If the ‘exit’ is blocked by gas, the ‘entrance’ (the esophagus) will feel more pressure. Regularly moving gas through the system can provide systemic relief.
Step-by-Step Gas Relief:
- The Bicycle: Lay baby on their back and gently cycle their legs toward their tummy. Do this at least 30 minutes after feeding.
- The ‘I Love You’ Massage: Using a baby-safe oil, trace the letters ‘I’, ‘L’, and ‘U’ on the baby’s abdomen to follow the path of the large intestine.
- Warm Compresses: A warm (not hot!) washcloth on the tummy can help relax the muscles of the LES.
The Importance of Tummy Time
While it seems counterintuitive, supervised tummy time during wake hours strengthens the core and neck muscles, which eventually helps the LES mature. Just ensure you wait at least 45 minutes after a feed before starting tummy time to avoid a ‘reflux volcano’!
When to Seek Medical Intervention

Red Flags Every Parent Should Know
Most cases of silent reflux are ‘developmental,’ meaning the baby will grow out of it by 6 to 9 months as they sit up and eat solids. However, sometimes medical help is necessary. Trust your gut, mama. If you feel something is wrong, it’s worth the call.
- Projectile Vomiting: If the ‘silent’ reflux becomes forceful, outward vomiting.
- Weight Loss: If the baby is dropping percentiles on their growth chart.
- Respiratory Issues: Wheezing, chronic cough, or any signs of labored breathing.
- Inconsolable Pain: If the baby is crying for more than 3 hours a day (Colic/Reflux overlap).
Your pediatrician may suggest a thickener for feeds or, in some cases, an H2 blocker or Proton Pump Inhibitor (PPI). These medications don’t stop the reflux, but they neutralize the acid so the ‘burn’ is gone, allowing the esophagus to heal.
Conclusion
You’ve Got This, Mama
Silent reflux is a test of endurance. It turns the ‘peaceful newborn phase’ into a series of tactical maneuvers and upright cuddles. But remember, every day your baby’s digestive system is maturing. By sticking to safe sleep surfaces, utilizing upright positioning, and mastering paced feeding, you are giving your baby the very best care possible.
Don’t forget to take care of yourself, too. The constant holding can be physically taxing. Use a baby carrier for those 30-minute upright sessions so you can keep your hands free and your back supported. You are the expert on your baby, and your steady, loving presence is the greatest comfort they have. Sleep will come again, the burn will fade, and soon these long nights will be a distant memory.





